
by Mahmoud Aljufaili
Introduction
Pneumothorax refers to the presence of air in the pleural cavity. It can impair oxygenation/ventilation. There are two types of spontaneous pneumothorax 1) primary, and 2) secondary. Primary refers to no underlying disease. Secondary refers to underlying pulmonary disease which has a worse prognosis.
Causes of secondary pneumothorax are various as follows;
- Vascular: Pulmonary infarct
- Airway disease: Asthma, COPD, Cystic fibrosis
- Neoplasm: Primary or metastatic
- Infective: Tuberculosis. Pneumocystis carinii pneumonia, lung abscess
- Interstitial lung disease: Sarcoidosis, Idiopathic pulmonary fibrosis
- Miscellaneous: Endometriosis
Risk factors increasing spontaneous pneumothorax risk;
- Family history
- Smoking
- Change in atmosphere pressure
- Marfans – in the absence of lung disease
Case Presentation
A 26-year-old male, with no significant medical history, presented to the emergency department with acute shortness of breath and associated right-sided chest pain. The pain started suddenly while the patient was at rest, it was sharp and worsening with inspiration. He denied a history of trauma, fever, cough or any other constitutional symptoms. In the ED, apart from tachypnea, his vitals were within normal limits. He was not in distress. The trachea did not deviate. Breath sounds were markedly diminished on the right side, with normal breath sounds on the left side. No wheeze or crackles were appreciated. The chest x-ray is shown below. What is your diagnosis and plan for this case?


Critical Bedside Actions and General Approach
- Assess the stability of the patient: Our first responsibility is to evaluate the patient vitals and control to airway, breathing, circulation abnormalities. In any instability, immediate actions are needed to stabilze the problem. Although there is a low chance to have a tension pneumothorax in spontaneous pneumothorax, this can be the worst case scenario for those patients. Oxygen, IV lines and cardiac monitorization may be necessary. Needle or tube thoracostomy can be necessary immediately on the bedside. These critical bedside actions are rarely needed for asymptomatic or mildly symptomatic patients. Therefore, we may have time to use proper diagnostic techniques for differential diagnoses.
- Size of pneumothorax: When we diagnosed pneumothorax, the patient symptoms are the driven factor for the treatment options. However, knowing the pneumothorax size is useful to decide the next step in majority of the cases. At least, today, the algorithms are still designed to the size of the pneumothorax.
- How to estimate the size of the pneumothorax?
- On the bedside, this can be done with Chest x-ray. It is ideal to get upright, postero-anterior, and inspirium-expirium x-rays. However, good quality, sitting antero-posterior bedside portable x-rays may guide us well.
- British Thoracic Society guidelines:
- If the interpleural distance at the level of the hilum i
- less than 1 cm, then it is a small pneumothorax
- 1 to 2 cm, then it is a moderate pneumothorax
- more than 2 cm, then it is a large pneumothorax
- If the interpleural distance at the level of the hilum i
- The American College of Chest Physicians
- If the distance from apex to cupola is
- Less than 3 cm, then it is a small pneumothorax
- More than 3 cm, then it is a large pneumothorax
- If the distance from apex to cupola is
- How to estimate the size of the pneumothorax?


- Primary or secondary
Differential Diagnoses:
The patients present mostly with shortness of breath (SOB). Therefore, pulmonary, cardiac and other causes of SOB should be considered first.
- Pulmonary
- Airway obstruction
- PE
- Pulmonary edema
- Anaphylaxis
- Asthma
- Cor pulmonale
- Aspiration
- Cardiac
- MI
- Tamponade
- Pericarditis
- Others
- Esophageal rupture
- Toxin ingestion
- Epiglottitis
- Anemia
If the pneumothorax is made clinically or radiologically, then the types should be confirmed as spontaneous, traumatic, primary, secondary or tension etc.
History and Physical Examination Hints
- Sudden pleuritic chest pain. Most often occur at rest.
- Increased work of breathing and tachypnea can be seen in moderate and severe pneumothorax.
- Hypoxemia can be seen in severe cases. Normal oxygen saturation does not rule out pneumothorax.
- Reduced breath sound on the affected side is more obvious with the increased size of pneumothorax (moderate or severe). Auscultation may not appreciate the difference in small pneumothorax, especially in a busy and noisy ED environment.
- Hypotension (think tension pneumothorax!). This is very important “red flag” for a pneumothorax patient. The patients are generally agitated because of hypoxemia and low blood supply to the brain. This finding should warn physicians to immediate action to treat the pneumothorax.
Emergency Diagnostic Tests and Interpretation
Chest X-ray
- Displaced visceral pleural line without lung markings between pleural line and chest wall
- Deep sulcus sign on supine x-ray
The Chest x-ray shows left side large pneumothorax with fully collapsed lung tissue. If the patient is vitally unstable (hypotensive, tachycardic, hypoxemic) and agitated, then this x-ray means “tension pneumothorax.” If the patient vitally stable, there is no tension. There is very important teaching point for all physicians. tension pneumothorax is a clinical diagnosis, not imaging diagnosis. Therefore, if the patient is clinically unstable and there is no breath sounds on the left side, this is tension pneumothorax until proven otherwise, and this x-ray should not be ordered. Nowadays, yes, you can use ultrasound in seconds to diagnose if you are in doubt.


Ultrasound
- No sliding lung sign
- Barcode (instead of the wave on the beach) appearance on M-mode (video)
The ultrasound clip below shows normal (left) and abnormal (right) lung findings. Lef side shows normal plura and lung tissue relation and called seashore sign. Right one shows no clear differentiation between these structure and look like a barcode. This finding is a warning for pneumothorax presence.
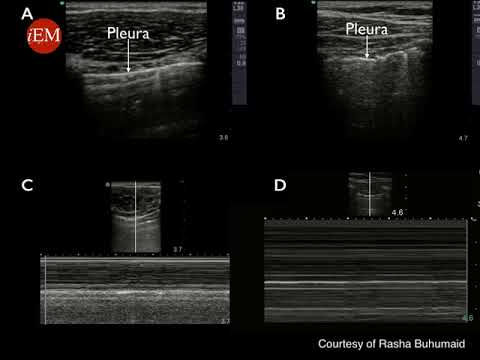
The ultrasound clip below shows “lung Point.” Please pay attention to hyperechogenic (white) line (pleura). Half of the pleura is moving, but other half is standing still (no lung sliding). The connection point is the border of pneumothorax line.

Computerized Tomography
- Very sensitive and specific
CT image shows left side pneumothorax, collapsed lung tissue.


Emergency Treatment Options
Initial Stabilization with oxygen, needle or tube thoracostomy (if necessary) is the the first priority for unsatble patients.
Oxygen: increase pleural air resolution by 3-4 times, and alone helps to absorbtion of the air by 1-2% a day. Therefore, some institutions may prefer to observe small pneumothoraxes with supplemental oxygen.
Procedures
Needle or catheter aspiration as effective as chest tube for small pneumothorax. Therefore, they are both appropriate treatment options. Although large pneumothoraxes may require tube thoracostomy, choosing the narrow tube size is effective as wide tubes. Most of the spontaneous pneumothorax are easily and safely treated with pig-tale catheters.
Needle decompression is necessary for tension pneumothorax. The classical teaching was 2nd intercostal space, mid-clavicular line, over the rib insertion. However, this location is recently controversial, especially in obese patients. Therefore, for adults, the new location is mid-anterior axillary line crossing with 4-5 th intercostal line. This location is also entry side of the chest tube. The below video demonstrates old version of needle decompression. However, this location is still acceptable in skinny adults and children.

The below video demonstrates chest tube insertion

The image shows left side chest tube location.


Disposition Decisions
Recurrent pneumothorax, the patient with abnormal vitals, bilateral pneumothorax, and all secondary pneumothorax should be admitted.
Small pneumothorax with no symptoms and normal findings can be discharged.
Please see the below algorithm below to understand possible treatments and disposition decisions.


If patients were discharged no flying for a week after resolution and no diving are standard recommendations.
References and Further Reading
- MacDuff A, Arnold A, Harvey J Management of spontaneous pneumothorax: British Thoracic Society pleural disease guideline 2010 Thorax 2010;65:ii18-ii31.
- Marx J, Hockberger R, Walls R, Biros M, Danzl D, Gausche-Hill M et al. Rosen’s emergency medicine.
- Tintinalli J, Kelen G, Stapczynski J. Emergency medicine. New York: McGraw-Hill, Medical Pub. Division; 2004.
- Daley BJ. Pneumothorax. (2017) https://emedicine.medscape.com/article/424547-overview – link