by Shaza Karrar
Case Presentation
A 39-year-old female presented to the emergency department (ED) complaining of right-lower-quadrant (RLQ) pain; pain duration was for 1-day, associated with nausea, vomiting, and loose motions. Abdominal pain started centrally and was described as diffuse and colic, 3 hours later it gradually shifted to the RL and became continuous in nature. Her Last-menstrual- period (LMP) finished a week ago. She denied any regular medications, known allergies or using any contraceptive pills. Also, she denied any past surgical history, travel history, or eating outside. Upon examination, she was found to be afebrile and vitally stable. The abdomen was soft, non-distended, with RLQ Tenderness, positive rebound tenderness, and positive bowel sounds.
General Approach and Critical Bedside Actions
General Approach and Key Concepts
Abdominal pain is a common complaint presented in the ED. It can range from benign, undifferentiated conditions to life-threatening ones. The role of the Emergency Physician (EP) is to identify life-threatening conditions for timely interventions. Life-threatening conditions can stem from various systemic pathologies (i.e. Cardiac, Gastrointestinal GI, Vascular, Urologic, Gynecologic, Infectious, etc.). As well, the EP has to assess properly and dispose of the less serious pathologies; which, if done poorly, can propagate and lead to delayed presentations and higher morbidities (i.e., Gastroesophageal reflux disease GERD, peptic ulcer disease, etc.). Special attention should be given to certain subgroups of patients including the elderly, the immunocompromised, females of childbearing age and children.
Types of Abdominal Pain
Abdominal pain can be either visceral, parietal or referred in origin (Table 1). In certain abdominal pathologies, abdominal pain can typically begin as visceral, dull and diffuse, and then progress to parietal, sharp and localizable, as in Appendicitis. Understanding the basic physiology of abdominal pain can be of immense aid in your assessment and approach.
Critical Bedside Actions
- A systematic approach, starting with a Focused Physical Examination and History Taking is key to reaching a diagnosis and consequently definitive management.
- Assessing the hemodynamic stability of the patient, pain score, and overall distress is a primary step in your approach, as it would set your pace as a clinician gathering bedside information and ultimately your workup and interventions (Figure 1).
- Keep in mind: You progress with assessing your patient’s stability, history taking and examination, all simultaneously, while advancing with any needed interventions that would stabilize your patient and alleviate his/her pain or distress.
- Do No Harm: Awareness of your limitations is extremely important. Acknowledging when your patient needs urgent assessment by your supervising senior, especially in an unstable patient, is part of your oath and a cornerstone of your practice during training years.
- Bedside actions are taken in patients presenting with abdominal pain and are tailored to each patient’s clinical picture; those include (Figure 2), detailed further in the chapter.
Differential Diagnoses
Abdominal pain can originate from intra-abdominal and extra-abdominal or non-GI conditions; hence, it’s advisable to be systematic in your approach to narrow down your differential diagnoses. (i.e., Cardiac, GI, infectious, hematologic, urologic, gynecologic, etc.) When diagnosing abdominal pain, the differential diagnoses can be based on anatomic localization of pain (Figure 3). This, in turn, helps direct your approach. An EP should prioritize possible life-threatening conditions in his differential diagnoses, and be mindful of other possible extra-abdominal causes attributable to abdominal pain (Table 2). Keep in mind that the following list of differentials is not exhaustive and should be correlated with the localization of abdominal pain (Figure 3).
History Taking and Physical Examination Hints
History Taking Hints
A properly focused history is of paramount importance, as it guides your physical examination, differential diagnoses, critical interventions, work up, and ultimately your disposition. Specific history findings can lead to prompt and accurate diagnosis and management.
History taking should cover the following
- General impression: level of distress, stability and pain scale.
- Patient Demographics: Gender, age.
- Onset and progression of pain: Sudden, gradual, episodic/intermittent, continuous.
- Localization of pain and radiations (Figure 3).
- The character of pain: Dull, sharp, colicky, stabbing, burning
- Severity: Pain Scale – mild, moderate, severe, or a scale from 1 to 10
- Alleviating and aggravating factors: Relieved by eating, sitting up, or worsens after eating, lying supine, movement, and coughing, etc.
- Associated symptoms: Be systematic – Fever, nausea, vomiting, loose-motions, melena, jaundice, dysuria, vaginal discharge/bleeding, shortness of breath, etc.
- Past medical, surgical and gynecologic/obstetric history: Known GI pathologies, chronic comorbid, recent trauma, previous similar complaint, previous surgeries, LMP
- Social history and Travel history: Alcohol consumption, illicit drug abuse, occupational hazards or exposures
- Medications and allergies history: Anticoagulants, corticosteroids, contraceptives.
- Others: Clues of an atypical presentation – considering Extra-Abdominal and non-GI pathologies including weight loss, unspecific systemic symptoms, etc.
Always try to screen for high-risk patients; certain history findings can help narrow your differential diagnoses. Table 3 demonstrates history findings, coinciding with their potential differentials.
Physical Examination Hints
A focused and systematic Physical Examination (P.E.) aims at verifying your clinical impression constructed from your history findings; it also aids in exposing unforeseen findings that may make you reassess your differential diagnoses and approach. Hence, an EP must have in mind specific working differentials obtained from the history before examining the patient (Figure 3 and Table 3). Make sure that your patient is comfortable with adequate pain relief as necessary, suitably positioned and appropriately exposed from nipples to lower abdomen/pubic-symphysis in a properly private environment. In the case of children, the presence of family members can aid your examination. Assessment of vital signs, hemodynamic stability, and signs of shock should be noted, keeping in mind that normal vital signs would not rule out a life-threatening condition.
Henceforth, a P.E. would be based on a focused and systematic approach, consisting of:
- General appearance and vital signs assessment:
- Note any instability in vitals, consciousness level, the posture of the patient, hydration status and signs of pallor, jaundice.
- Examination of extra-abdominal systems:
- Entails an assessment of the cardiorespiratory functions.
- Other extra abdominal systems of suspicion attributing to the patient history and clinical picture.
- Focused abdominal examination:
- Inspection: Distention, surgical scars, masses, distended veins, skin discoloration.
- Palpation:
- The light then deep palpation begins with the opposite non-tender quadrant, progressing through all quadrants.
- Assess for tenderness, guarding, rebound tenderness, hepatosplenomegaly, and masses; for instance, a rigid, tense abdomen with involuntary guarding is highly indicative of peritonitis. Look for costovertebral angle tenderness and palpate
- Look for costovertebral angle tenderness and palpate bimanually for renal masses.
- Percussion: Dullness for ascites or Resonance.
- Auscultation: Hyper/hypoactive or absent bowel sounds and vascular bruit.
- Specific signs and maneuvers: (Table 4)
- For an overview of the focused Abdominal Examination, please watch the following video.
- Serial abdominal examinations are important to reassess your patient’s progress and response to treatment.
- Rectal examination: In suspected GI bleeds, perianal and prostatic disease, foreign bodies, and impacted stools.
- Examination of hernial orifices: All should be cleared; easily missed in the exam.
- Genital and pelvic examination:
- Pelvic exam in all females with lower abdominal pain and query pelvic pathologies.
- Genital exam in males with possible testicular pathologies and hernias.
Emergency Diagnostic Tests and Interpretation
Bedside tests
- 12-lead ECG
- Initial screening for cardiac pathologies (i.e., Acute Coronary syndrome; MI, AFib, Digoxin toxicity, etc.), especially in patients presenting with epigastric pain, cardiovascular risk, and elderlies with poorly localizable pain. Consider follow-up cardiac enzymes in high-risk patients and abnormal ECG findings.
What is your opinion about below ECG in a patient with abdominal pain?

- Urine Pregnancy test: All females of childbearing age, regardless of history findings
- Urine analysis: Signs of hematuria or Urinary Tract Infections (UTI).
- Capillary Glucose test: Hyper/Hypoglycaemia and DKA
- Ultrasound
- Considered the new EP stethoscope – bedside, non-invasive, yet operator-dependent
- Aids at assessing solid abdominal organs, the presence of intraperitoneal fluid, vascular and hemodynamics of the patient
Laboratory tests
- Complete-Blood-Count: Leukocytosis, Hemoglobin level, Platelets count
- Electrolytes: Correct any derangements caused by fluid losses.
- Blood-Urea-Nitrogen (BUN): Assess dehydration.
- Creatinine / Renal Function: Assess renal functions, dehydration, and record a baseline in case of needed contrast imaging studies to prevent possible contrast-induced-nephropathy.
- Liver function test (LFT): Liver and gallbladder pathologies
- Amylase: Increased in most intra-abdominal pathologies.
- Lipase: Levels twice the normal is highly indicative of pancreatitis, joined with elevated LFT, could raise the suspicion of Gallstones pancreatitis.
- Inflammatory markers: CRP or Procalcitonin
- Coagulation profile: Patient on anticoagulation (i.e., Warfarin for AF) – if reveals sub-therapeutic levels, would raise suspicion of mesenteric ischemia, or if supra-therapeutic, would raise suspicion of active bleed, as well a standard test for possible surgical interventions; in need of reversal.
- Quantitative hCG Blood: Confirmatory after a urine pregnancy test
- TestType and screen: For all patients possibly proceeding for surgical interventions
- Rh Status: All female patients with possible ectopic pregnancy
Imaging modalities
X-rays
- An initial imaging modality, quick yet not very sensitive
- Chest X-rays: Delineate Air under the diaphragm in perforated viscus or pneumonia.
- Abdominal X-rays: Usually in erect and decubitus positioning; looking for Bowel distention, air-fluid levels, obstruction, foreign bodies.
What is your opinion about below abdominal x-ray in a patient with abdominal pain?

Ultrasound (US)
- Extended sonographic studies can further your assessment; considered the study of choice in pregnant women.
- Abdominal US: Evaluation of biliary tract pathologies, intraabdominal organs, and free intraperitoneal fluid, Intussusception, appendicitis, etc.
What is your opinion about below ultrasound samples in a patient with abdominal pain?


- Kidney-Ureter-Bladder KUB US: Nephrolithiasis, hydronephrosis, urine retention, etc.
- Pelvic or Obstetric US: Tubo-ovarian pathologies, intrauterine and ectopic pregnancy, fibroids, etc.
- Testicular US: Testicular torsion, epidedimo-orchitis
- Vascular US Studies: assessment of the abdominal aorta
Computed tomography (CT) scan: (With/Without Contrast, Angiography)
- Highest in sensitivity and specificity in detecting most common pathologies
- Ionizing and considered limited in the case of contrast allergies, pregnancy, or pre-existing renal insufficiency predisposing the patient to contrast-induced nephropathy.
Magnetic resonance imaging (MRI):
- Limited use in the ED, considered in pregnant patients of inconclusive US findings.
Emergency Treatment Options
Initial Stabilization
- Primary survey: Hemodynamic stability assessment subsequently sets the pace of your approach (Figure 1).
- Secondary survey: Identify life-threatening conditions (Table 2), and screen for the high-risk patients, and special age groups (Table 3).
- Hemodynamically unstable patients should be resuscitated without any delay, entailing the following keystones (Figure 4).
- Appropriate surgical consultations should be sought in a timely manner, especially in the hemodynamically unstable patient and surgical conditions in need of an intervention.
- A hemodynamically stable patient should be properly worked up and reassessed frequently, as he/she may deteriorate and become unstable.
- Patients with possible peptic ulcer disease (PUD) and gastritis can benefit from a “GI cocktail,” typically constituted of a combination of antacid, viscous lidocaine, and antispasmodics.
- Otherwise, stable patients who are responsive to treatment, with conditions of low acuity, can be fit for discharge from the ED with an appropriate disposition and follow-up plan.
Medications
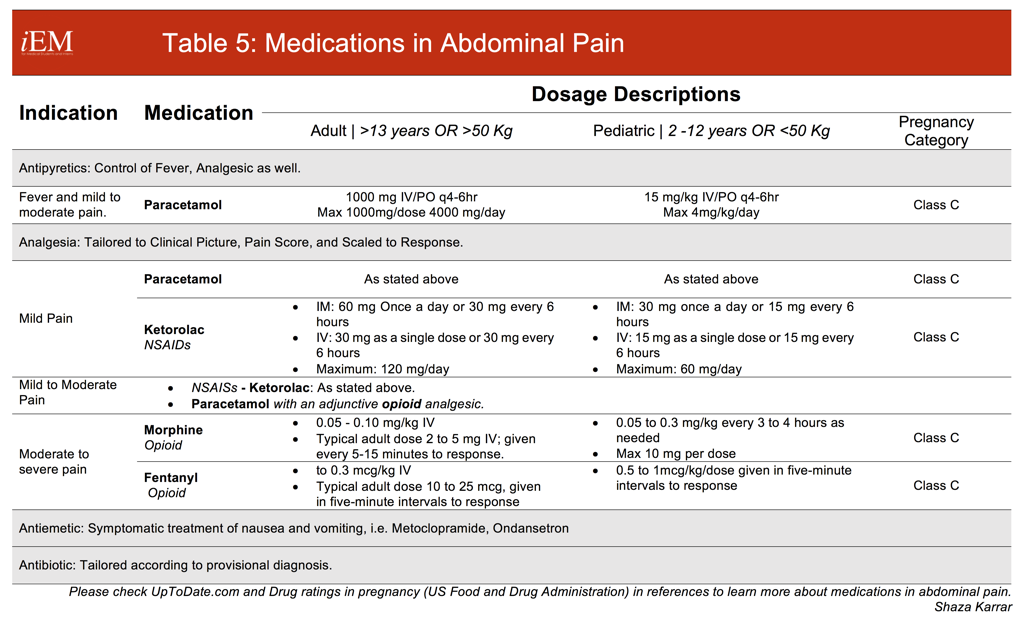
- Analgesics should be tailored to each patient’s clinical picture, pain score, and response, with an aim to relieve his distress and pain to a manageable level, making him more comfortable and cooperative for the abdominal exam and reassessment (Table 5).
- Abdominal pain should be addressed with liberal analgesia, including the use of opioids, as it has been recently proven that they do not alter physical exam findings or increase the number of incorrect management decisions.
- Opiate-dependent patients and chronic users may need higher doses for an adequate response.
- Always monitor patients for respiratory depression with opioids and always consider dose adjustments in geriatrics and patients with renal and hepatic impairments.
- NSAIDs like Ketorolac are suitable for biliary and renal colic but not in PUD.
{kind=link}
Procedures: None
Pediatric, Geriatric, Pregnant Patient and Other Considerations
Pediatric Patient
- The list of differential diagnoses tends to rearrange in acuity according to the age at presentation in pediatric patients. For example:
- 0 to 3 months: testicular torsion, necrotizing enterocolitis, incarcerated hernia and pyloric stenosis
- 3 months to 3 years: intussusception, vaso-occlusive crisis, UTI and toxic megacolon, among those just stated above
- 3 years to adolescence: appendicitis, mesenteric lymphadenitis, DKA and toxic ingestion, as well among those just stated above
- When it comes to examining for peritoneal sign in pediatrics, children can be asked to jump up and down as an indirect means of inciting peritoneal irritation.
Geriatric Patient
- Elderly and immunocompromised patients deserve special attention as a higher risk group compared to their younger counterparts; they are more likely to present late in the disease process and with atypical presentations.
- The elderly commonly present with multiple comorbidities, difficult communication skills, and vague symptoms that are not reflective of the actual severity of their disease.
- It’s important to establish their medication and allergies history (Anticoagulants, etc.)
- They cannot tolerate volume loss and hence can deteriorate easily, and their abdominal exam is often unspecific; however, they’re the most likely population to have surgical emergencies.
Pregnant Patient
- Females of childbearing age presenting with abdominal pain are presumed to have an ectopic pregnancy until proven otherwise, regardless of their history.
- Pregnant women are at risk of the same abdominal conditions as all other patients, but they propose special considerations.
- Restricted imaging necessitates astute work up and reassessment.
- Consider first-trimester abortion in abdominal pain in a pregnancy < 20 weeks of gestation.
- In pregnant women well advanced in their pregnancy, consider obstetric emergencies, such as Preterm-Labor, Placenta Previa and abruption, Uterine Rupture and HELLP syndrome.
Other considerations
- Appendicitis should be considered in all patients presenting with acute abdominal pain, refer to Alvarado Score.
- Abdominal trauma, blunt and penetrating, results in a myriad of intraabdominal injuries that shouldn’t be taken lightly but well investigated and addressed.
Disposition Decisions
Admission criteria
- Hemodynamically unstable patients require admission to the Intensive Care Unit (ICU), especially post possible surgical interventions.
- Elderly patients with multiple comorbidities or anticipated clinical course deterioration require an ICU admission as well or a High Dependency Unit (HDU) if available.
- Hemodynamically stable patients found to have surgical conditions can be admitted to a general ward.
- The conservative and low threshold for admission is strongly advised and advocated in the high-risk groups.
- Certain stable patients might need to be admitted for further evaluation and planned interventions.
Discharge criteria
- Patients who are responding to treatment, with a resolution of symptoms, without signs of underlying life-threatening conditions, can be discharged.
- Always instruct your patients to return to the ED in the case of progression of abdominal pain or worsening general condition, which is not getting relieved, such as persistent vomiting, jaundice, fever, etc.
- Patients with an unclear etiology of pain who are stable enough for discharge should be reassessed again within 12 to 24 hours; hence, a follow-up plan should be instituted and emphasized to the patient.
Referral
- Follow up plans in patients that are discharged decrease high morbidity and mortality, a chance of a missed diagnosis, and decrease unnecessary ED presentations of benign and low acuity abdominal pain.
- Follow up plans are essential and have to be arranged for certain patients. Those include:
- Patients in need of the re-evaluation of their symptoms’ progression and resolution; particularly patients at higher risk.
- Patients with an unclear pathology that needs a further workup by multidisciplinary services – vascular, urology, OB/GYN, gastroenterology, etc.
- Patients with known GI pathologies or comorbidities, who did not follow-up, are in need of reinstitution of their primary or specialty care.
- Pregnant women should resume their primary care obstetricians, with an advised reassessment as soon as possible post discharge.
- Yet pregnant women are strongly instructed to return to the ED in case of recurred, progressing or persistent symptoms, especially in cases of uncorrected volume loss due to vomiting and loose motions, vaginal bleeding/discharge, and abdominal pain.
References and Further Reading
- O’Brien M. C. Acute abdominal pain. In: Tintinalli J. E., Stapczynski JS, Ma OJ, Cline DM, Cydulka, RK, Meckler GD. Tintinalli’s Emergency Medicine: A Comprehensive Study Guide. 7th ed. New York, NY: McGraw-Hill, 20 11, pp. 519-527
- Gavin R. Budhram, Rimon N. Bengiamin, Abdominal Pain. In: A. Marx J. S. Hockberger R., M. Walls R., et al. Rosen’s Emergency Medicine: Concepts and Clinical Practice. 8th ed. Philadelphia: Saunders, an imprint of Elsevier, 2014, pp. 223 – 2231.e1
- Chai Chan K., Seow E. Approach to abdominal pain. In: C. Peter., J. George, K. Anne-Maree, B. Anthony Brown, M. Little. Textbook Of Adult Emergency Medicine. 4th ed. Elsevier, 2015, pp.329-337
Links to More Information
- iEM-Biliary Disease – link
- iEM-AAA-link
- iEM-Acute Appendicitis – link
- iEM-Viscus perforation – link
- iEM-Ectopic pregnancy – link
- iEM-ACS-link
- iEM-Acute mesenteric ischemia – link
- iEM-Massive GI bleeding – link
- Abdominal Examination – Accessed on date 16th of June 2016
- CDEM Curriculum – Abdominal Pain
- EMclerkship – Abdominal pain part-2 (audio)
- Skeptics’ Guide to Emergency Medicine: podcast and blog post- Accessed on 16th June 2016
- Life in the Fast Lane: Trauma! Assessing the Abdomen – by Chris Nickson, Accessed on 16th June 2016
- R.E.B.E.L-em: Is Pelvic Exam in the Emergency Department Useful? – by Salim Rezaie, Accessed on 16th June 2016
Others
- Table 4: Modified version adapted from: Chai Chan K., Seow E. Approach to abdominal pain. In: C. Peter., J. George, K. Anne-Maree, B. Anthony Brown, M. Little. Textbook Of Adult Emergency Medicine. 4th ed. Elsevier, 2015, Table in pp.332, Originally adapted from: White MJ, Counselman FL. Troubleshooting acute abdominal pain Emedmag. 2005.
- Ranji SR, Goldman LE, Simel DL, Shojania KG. Do opiates affect the clinical evaluation of patients with acute abdominal pain? JAMA 2006; 296:1764.
- All medications (Table 5) references and dosages were obtained from
- UpToDate.com
- Drug ratings in pregnancy (US Food and Drug Administration): Obtained from UptoDate
The video associated to the lecture has been deleted, is it possible to repost it?
Which video to be exact?