by Kuan Win Sen
Case Presentation
A 62-year-old man presents to the ambulatory area of the emergency department complaining of sore throat, fever, and chills. He has history of type 2 diabetes mellitus, hypertension, and obesity. He was seen by the general practitioner (GP) 2 days prior and was prescribed thymol gargle and paracetamol. Further history reveals progressive difficulty and pain in swallowing, decrease in appetite, and worsening sore throat since the GP visit two days ago. On physical examination, he is alert, has a temperature of 39.1C, heart rate of 112 per minute, blood pressure of 136/74mmHg, respiratory rate of 18 per minute and oxygen saturation of 98% on room air. He speaks with a muffled voice and has drooling of saliva. There are no obvious findings in the oropharynx and no cervical lymphadenopathy. The rest of the physical examination is unremarkable.
Critical Bedside Actions and General Approach
Every patient who presents to the ED will receive initial bedside evaluation (ABC…), and vital signs check. Depending on the history and general look of the patient, our first priority is to evaluate some symptoms and signs of impending airway obstruction. This evaluation can be done in the triage or inside the ED. If there are findings, the patient should be triaged to high acuity area. Airway equipment and monitoring devices should be placed to the patient. Depending on the patient’s initial evaluation, any abnormality found in ABC evaluation should be treated immediately. However, suspicion of epiglottitis may change some management strategies such as involving airway specialists earlier.
Differential Diagnoses
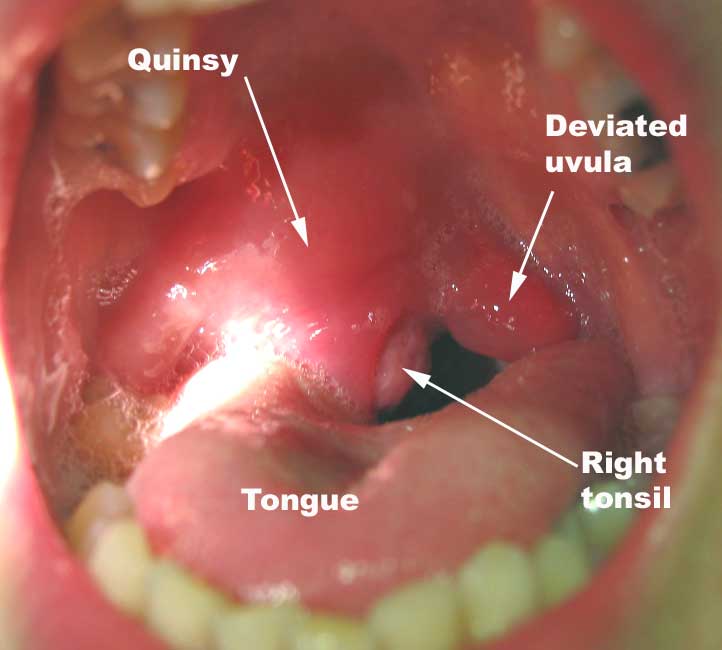
- Peritonsillar abscess (quinsy)
- Diphtheria
- Submandibular space infection (Ludwig’s angina)
- Laryngotracheitis (croup)
History and Physical Examination Hints
Have a high index of suspicion for epiglottitis in patients reattending ED for worsening sore throat. Severe sore throat with odynophagia, high fever, muffled voice (“hot potato voice”) and drooling are common clinical features of epiglottitis. Patients with impending airway compromise would refuse to lie down for examination. Suspect epiglottitis if the severity of sore throat is out of proportion to findings in the oropharyngeal examination.
- Assess the soft palate for swelling and/or deviation of the uvula to exclude peritonsillar abscess (quinsy)
- Assess the sublingual and submandibular regions for swelling to exclude Ludwig’s angina
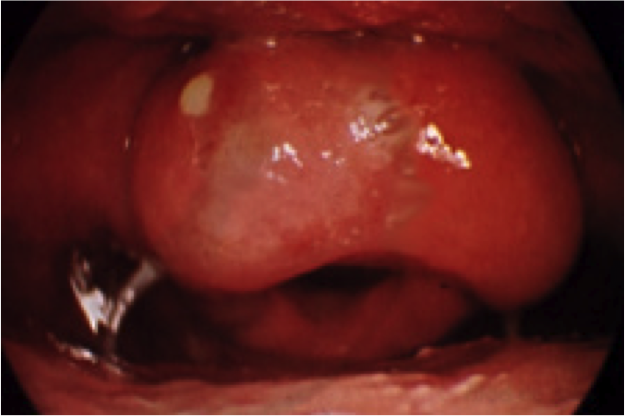
- Assess the tonsils for grey pseudomembranes that are classically seen in diphtheria
Patients with croup have a “barking” cough and are generally comfortable in the supine position.
Emergency Diagnostic Tests and Interpretation
- Obtain a lateral neck X-ray (“thumb” sign)


Typical findings of epiglottitis with enlarged epiglottis and aryepiglottic folds.
- Prepare for laryngoscopic visualization using a flexible nasolaryngoscopy (gold standard).
- Diagnostic laboratory investigations (complete blood count and blood culture) should not be performed in patients where suspicion of epiglottitis is high until the airway is secured.
Emergency Treatment Options
- Airway maintenance is paramount
- Provide humidified supplemental oxygen
- Consider prophylactic intubation to secure the airway in progressive disease
- Prepare the surgical airway set for the possibility of encountering a difficult airway
- Avoid supraglottic devices as they may compress the swollen epiglottis
- Administer antibiotics (intravenous ceftriaxone 2g and intravenous clindamycin 600mg)
- Other options such as Racemic epinephrine, eta-agonists, and corticosteroids have not been shown to be beneficial in epiglottitis treatment.
Pediatric Considerations
- Epiglottitis used to be more common in children with incomplete or lack of Hib immunization. However, the adult to child ratio has increased since the turn of the century.
- Typical findings in children:
- Look toxic
- Reluctant to lie down
- Classical drooling, dysphagia, distress (3D’s)
- Tripod position
- Sniffing position
- Individualize examination according to the severity of illness
- those with classic symptoms of epiglottitis or stridor should have involvement of pediatric airway experts before attempts at visualization as there have been reports of cardiorespiratory arrest in children during these attempts
Disposition Decisions
Intubated patients or those who require very close monitoring should be admitted to the surgical intensive care unit or high dependency unit.
References and Further Reading
- Shah RK, Stocks C. Epiglottitis in the United States: national trends, variances, prognosis, and management. Laryngoscope. 2010;120:1256–1262.
- Ovnat Tamir S, Marom T, Barbalat I, Spevak S, Goldfarb A, Roth Y. Adult supraglottitis: changing trends. Eur Arch Otorhinolaryngol. 2015:272(4):929-35
- Guldfred LA, Lyhne D, Becker BC. Acute epiglottitis: epidemiology, clinical presentation, management and outcome. J Laryngol Otol. 2008;122(8):818-23.
- Ward MA. Emergency department management of acute respiratory infections. Semin Respir Infect 2002; 17:65.
- McEwan J, Giridharan W, Clarke RW, Shears P. Paediatric acute epiglottitis: not a disappearing entity. Int J Pediatr Otorhinolaryngol 2003; 67:317.
- Medscape – epiglottitis medication – Gompf SG (2018) – link
Links To More Information
Videos
- Flexible nasolaryngoscopy demonstrating enlarged epiglottis and aryepiglottic folds (https://www.youtube.com/watch?v=f-iKuIN7x6E)
- “Barking” cough characteristically heard in croup, that is most commonly seen in children (https://www.youtube.com/watch?gl=SG&v=Qbn1Zw5CTbA&hl=en-GB)
Pictures/Images
- Peritonsillar abscess – swelling of the right peritonsillar fold with deviation of the uvula to the left (http://1.bp.blogspot.com/-ETI_7tws-Mk/T00p3R3zCFI/AAAAAAAAC78/8NYqI1YWkk0/s1600/quinsy1.jpg)
- Ludwig’s angina is cellulitis of the floor of the mouth (http://cosmos.phy.tufts.edu/~rwillson/dentgross/headneck/ludws.jpg)
- Diphtheria – adherent, dense, grey pseudomembrane covering the tonsils (https://upload.wikimedia.org/wikipedia/commons/4/47/Dirty_white_pseudomembrane_classically_seen_in_diphtheria_2013-07-06_11-07.jpg)
- “Thumb” sign on lateral neck X-ray showing the enlarged epiglottis (http://images.radiopaedia.org/images/3345568/7c6478defa226b1899da09938600e5_big_gallery.jpg)
- Enlarged epiglottis seen on flexible nasolaryngoscopy (http://coreem.net/content/uploads/2015/07/Epiglottitis-2.png)
- A child demonstrating the “tripod” position to improve diaphragmatic excursion (http://airway.jems.com/wp-content/uploads/2011/10/evolving-assessment6.jpg)
- A child demonstrating the “sniffing” position to maximize air entry (https://pedclerk.bsd.uchicago.edu/sites/pedclerk.uchicago.edu/files/uploads/images/m_20052.011.019B_1_0.jpeg)
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}