

Burnout is a form of distress that manifests with features of emotional exhaustion, depersonalization, and reduced personal/professional accomplishment. Emotional exhaustion or unsuccessful coping with stressors, is the fatigued feeling that develops as one’s emotional energies are drained. Depersonalization refers to a student’s indifference, negative or cynical attitude. Reduced personal accomplishment is a negative self-evaluation of one’s abilities which manifests itself with feelings of failure. University education is an intrinsically demanding time which puts university students at risk for burnout, coupled with other burnout risk factors such as individual/personal factors and extracurricular factors. Burnout causes significant physical, emotional, psychological, and spiritual damage to students.
However, from this article there had been paucity of and discrepancies in data on the overall prevalence of burnout in university students from low- and middle-income countries (LMICs). Students pursuing health-related programs in mostly high-income countries (HICs) had been mostly studied previously.
In this review, 55 articles were included, with a total of 27,940 (female: 16,215, 58.0%) university students from 24 LMICs. The Maslach Burnout Inventory (MBI) was found to be the most widely used tool for measuring burnout in 43 studies (78.2%). The pooled prevalence of burnout was 12.1% (95% CI: 11.9–12.3; p = < 0.001). Pooled significant prevalence of emotional exhaustion, cynicism, and reduced personal/professional efficacy were 27.8% (95% CI 27.4–28.3), 32.6% (95% CI: 32.0– 33.1), & 29.9% (95% CI: 28.8–30.9) respectively. Burnout pooled prevalence was highest among the African region at 35.4%, followed by the Asian region at 30.2%, and the European region at 20.7%.
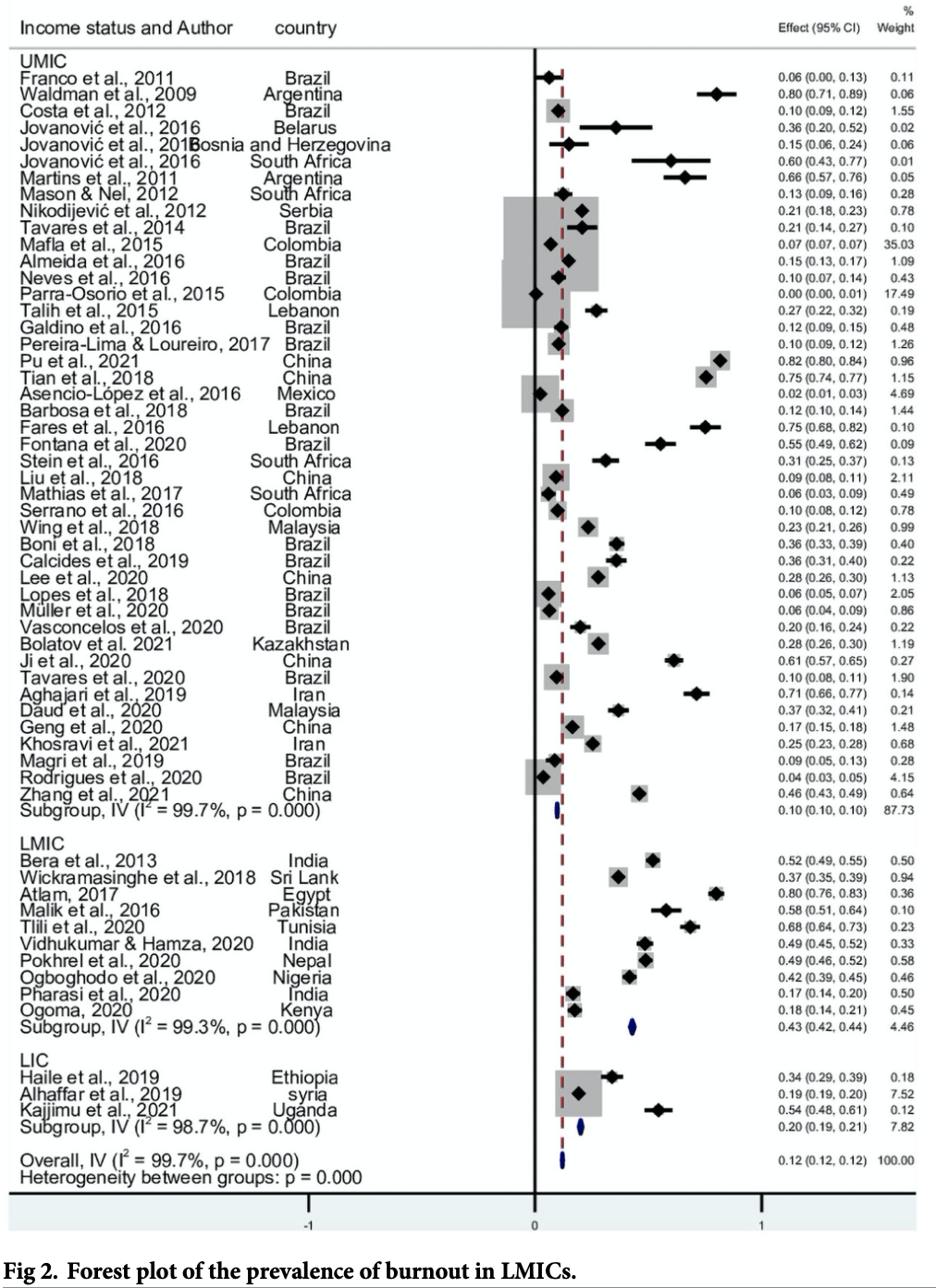
Figure 1: Forest plot for the prevalence of burnout in LMICs
In this review, burnout rates found in LMICS were lower than those in HICs, which the author believed to be due to publication bias. Authors further recommended low cost interventions that were needed more in low income countries than in middle income countries for managing burnout. These included mindfulness practices, yoga exercises, and group discussions. The current COVID-19 pandemic was also highlighted as having been found to put university students at a higher risk of burnout. Consequences of burnout in students include absenteeism, drop out, reduced academic performance, depression, alcohol and drug abuse, suicide, professional impairment and dissatisfaction, increased incidence of errors and near-misses.
























